
Hyperacusis
Hyperacusis is a condition characterized by an abnormally heightened sensitivity to everyday sounds that are typically well tolerated by others. People with hyperacusis may perceive normal environmental noises (such as running water, clinking dishes, or voices) as uncomfortably loud, intrusive, or even painful. This reaction occurs due to a dysregulation within the auditory system, where sound processing pathways become overly reactive. In some cases, there may also be structural changes in the middle ear, and an emerging theory proposes hypermobility of the stapes as a contributing factor.
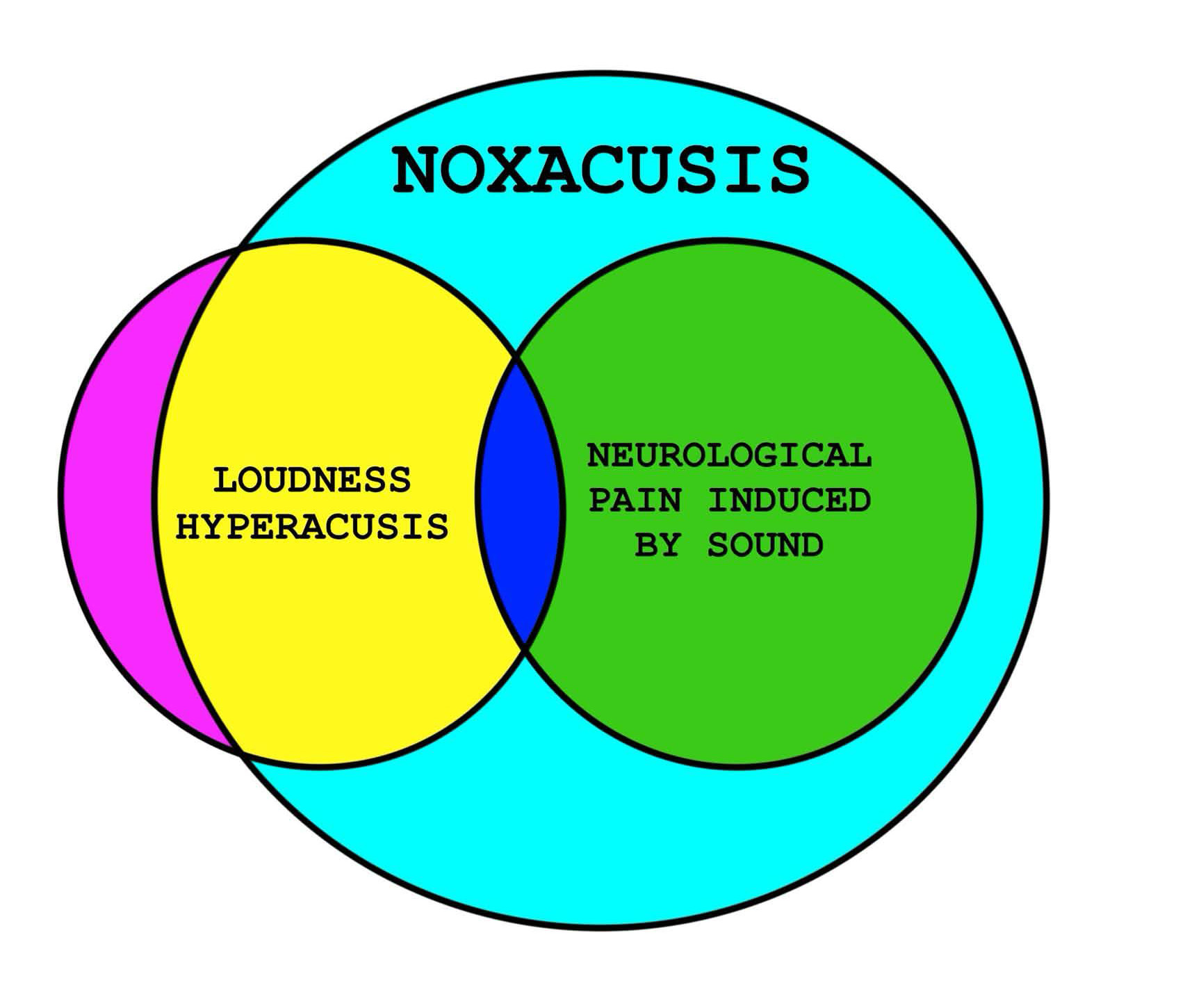
- Noxacusis: Any form of ear pain caused or worsened by sound. Noxacusis is a term that encompasses both primary loudness hyperacusis and neuralgia-related sound sensitivity.
- Primary loudness hyperacusis: Reduced sound tolerance due to a dysregulation within the auditory system, where sound processing pathways become overly reactive. Normal environmental sounds are perceived as uncomfortably loud or intrusive, and disomfort or pain (noxacusis) may be present in more advanced cases.
- Neuralgia-related sound sensitivity: Heightened sound sensitivity which develops alongside or secondary to neuropathic pain (neuralgia). Although still considered a form of noxacusis, neuralgia-related sound sensitivity is thought to arise from hypersensitization of cranial nerves innervating the ear and face, leading to amplification of sensory input and increased auditory discomfort.
Hyperacusis often follows acoustic trauma or prolonged noise exposure and its severity can vary widely. For many individuals, hyperacusis causes distress, anxiety, and social withdrawal as they attempt to avoid environments that provoke discomfort. Proper management should focus primarily on protecting against harmful sound exposure. Once auditory tolerance shows signs of improvement, sounds can be carefully and gradually reintroduced in a controlled environment.
The key features of hyperacusis include reduced sound tolerance, tinnitus (often reactive), and discomfort or pain in more advanced cases. When pain or discomfort is present, it is often accompanied by a sensation of aural fullness or pressure. These symptoms typically worsen after exposure to sounds above the individual’s tolerance threshold. In the earlier and milder stages, pain is often absent, recovery from setbacks is quicker, and sound tolerance usually returns to baseline. However, in severe cases, pain becomes a persistent feature, and any setback can cause a lasting reduction in sound tolerance. Recovery in such cases tends to be slow and difficult, with some individuals experiencing setbacks that seem permanent or last for years.
At Hyperacusis Guide, we have reviewed hundreds of patient cases and, in most instances, communicated directly with the patients to better understand the details of their symptoms. Through this process, we have observed that many patients, researchers, and clinicians describe hyperacusis and noxacusis as two distinct conditions, yet the definition of noxacusis in the literature is often vague. In our view, noxacusis represents a more severe form of loudness hyperacusis in which pain is also present. We have also identified a subset of patients who are not well described in the existing literature, specifically those with neuropathic-related pain and sound sensitivity, and we believe these individuals also fall under the noxacusis category.
We use noxacusis as an umbrella term that refers to any form of ear pain caused or worsened by sound. Within this umbrella, we believe there are two distinct subtypes:
- Severe loudness hyperacusis with pain: This occurs when loudness hyperacusis becomes severe enough that sound begins to cause pain. In these cases, noxacusis represents a painful progression of hyperacusis rather than a separate disorder. Pain may occur immediately when sound exceeds the individual’s tolerance threshold or may be delayed by hours or days. Once triggered, symptoms can persist for weeks, months, or even years, and often fluctuate in intensity. The pain is typically focused and localizes to the middle ear (deep to the tympanic membrane), is often sharp or stabbing, and may be accompanied by a sensation of aural fullness or pressure.
- Neuralgia-related sound sensitivity: This occurs when heightened sound sensitivity develops alongside or secondary to neuropathic pain (neuralgia). Although still considered a form of noxacusis, neuralgia-related sound sensitivity is thought to arise from hypersensitization of cranial nerves innervating the ear and face, leading to amplification of sensory input and increased auditory discomfort. Patients often report burning, aching, or stabbing pain around the ear that may radiate into the face or head. Individuals in this group may experience these neuropathic symptoms without major signs of traditional hyperacusis, such as loudness intolerance, aural fullness, or worsening overall condition from sound. Based on our observations, these patients may respond better to medications such as clomipramine than those with primary loudness hyperacusis.
Note: There may be some overlap between these two subtypes of noxacusis, and it is possible for an individual to display symptoms from both groups simultaneously, but most people still tend to fall primarily into one group.
Lastly, we believe it is extremely important for individuals who are newly affected by hyperacusis to avoid sound therapy and tinnitus retraining therapy (TRT), at least until their symptoms have stabilized and they have a clear understanding of their tolerance thresholds. We recommend practicing sound isolation during the early stages of recovery until these limits are better understood. The recovery process can take some time and should not be rushed. Individuals may need to make significant lifestyle adjustments and, in some cases, temporarily or permanently stop working to avoid worsening their symptoms.
Key Features of Hyperacusis
- Reduced sound tolerance, tinnitus (often reactive), and discomfort or pain in more advanced cases. When pain or discomfort is present, it is often accompanied by a sensation of aural fullness or pressure.
- Noxacusis is a term that encompasses both loudness hyperacusis and neuropathic-related sound sensitivity.
- Primary loudness hyperacusis is a distinct condition from neuropathic-related sound sensitivity.
- Can lead to social withdrawal and isolation to avoid sound exposure. Severe cases are usually completely homebound.
- Often follows acoustic trauma or prolonged noise exposure.
- Sometimes associated with tonic tensor tympani syndrome (TTTS).
Hyperacusis Severity Scale
At Hyperacusis Guide, we noted the lack of a standardized severity grading system for hyperacusis. To address this gap, we propose the following severity scale, intended to enable consistent classification, assist clinical management, and enhance the quality of data collected for research. Note that pain is not included as a metric in this severity scale, as it is a subjective measure and may be reported inconsistently among individuals with hyperacusis.
- Can generally function day-to-day with adaptations.
- Requires hearing protection in louder environments (e.g., restaurants, shopping, public events).
- Avoids certain activities that are uncomfortably loud.
- May still manage quiet activities or maintain a quiet job.
- Symptoms interfere significantly with work and daily activities.
- May have to stop current employment or change to a low-noise job.
- Often makes a choice to be primarily homebound to not worsen, leaving mainly for doctor visits or necessities, which is something they still have tolerance for.
- Social activities and travel are very restricted.
- Hearing protection is needed for almost all situations outside the home.
- Unable to tolerate many ordinary sounds, often including normal conversation.
- Requires hearing protection for most things in and out of the home.
- Talking, household sounds, and minimal daily activity provoke strong symptoms.
- Homebound has become absolutely mandatory to not worsen.
- Those in this category do not leave home at all, or not for very long periods of time, and typically only in life-or-death or extremely pressing situations.
Misophonia and Phonophobia
Hyperacusis, misophonia, and phonophobia are all conditions involving abnormal sound sensitivity, but they differ significantly in their underlying mechanisms, emotional responses, and clinical features.
Hyperacusis is a physical intolerance to everyday sounds that are perceived as uncomfortably loud or even physically painful. It reflects an increased sensitivity within the auditory system, meaning the ear or brain reacts more strongly to sound than normal. As a result, ordinary sounds can cause pain, pressure, or discomfort for the individual.
Misophonia, in contrast, involves strong emotional and behavioral reactions such as anger, anxiety, or disgust in response to specific “trigger” sounds like chewing, breathing, or tapping. The reaction is not related to how loud the sound is, but rather to its particular pattern or context, as the brain interprets certain sounds as intrusive or highly unpleasant.
Phonophobia is characterized by a fear-based or anticipatory response to sound. Individuals with phonophobia experience anxiety or dread in anticipation of certain sounds, often because because they expect those sounds to be unpleasant or overwhelming. It is primarily an anxiety-related condition, where the fear of sound itself leads to avoidance or distress in everyday environments.
Although the Loudness Discomfort Level (LDL) test is sometimes used to differentiate these conditions, we do not recommend it for individuals with hyperacusis. During the test, harsh pure-tone beeps are played at gradually increasing volumes until the individual indicates the sound is uncomfortably loud, which can dramatically worsen symptoms. Furthermore, the LDL test is unreliable and provides little to no clinical benefit.
- The test is not standardized, objective, or accurate.
- LDLs cannot be relied upon to represent a person’s ability to tolerate sound in daily life.
- LDLs and self-ratings of decreased sound tolerance are poorly correlated.
- LDL testing can permanently worsen tinnitus and hyperacusis symptoms, and offers little to no meaningful clinical benefit.
- The test uses harsh, pure-tone beeps at various frequencies. These tones are directed into an already injured ear, eliciting the same discomfort the patient is seeking help for.
- Patients tested are often those least likely to be comfortable with LDL testing.
- Patients have the right to decline LDL testing or any test.
Individuals with hyperacusis typically have significantly lower LDLs (often 70–90 dB or lower), reflecting reduced tolerance for sound intensity.
Individuals with misophonia usually have normal LDLs, since their discomfort arises from emotional or contextual responses, not loudness.
Those with phonophobia may have normal or near-normal LDLs, but they often avoid sound due to fear or anticipation of discomfort rather than actual auditory pain thresholds.
Individuals on the autism spectrum often experience heightened sensory sensitivities, and studies suggest that approximately 12.8% to 35.5% of those with autism spectrum disorder (ASD) may also meet criteria for misophonia or phonophobia. However, it is important to recognize that hyperacusis is a distinct condition and should not be confused with misophonia or phonophobia. Many healthcare providers unfamiliar with hyperacusis may mistakenly assume that patients with sound intolerance are experiencing misophonia or anxiety-related sound aversion.
This distinction is important because many reported “success stories” with sound therapy likely involve patients who actually had misophonia, phonophobia, or very mild hyperacusis that was capable of improving on its own. These cases respond to sound therapy not because it treats true sensory or pain-based sound intolerance, but because their underlying issue is psychological or behavioral rather than auditory or nociceptive.
Hyperacusis
- Physical intolerance to normal sounds.
- Everyday sounds are perceived as uncomfortably loud or even physically painful.
- Involves abnormal auditory gain or nerve sensitivity.
- May involve structural changes in the middle ear (hypermobility of the ossicles).
- Frequently associated with tinnitus (often reactive tinnitus).
- Often follows acoustic trauma, prolonged noise exposure, or ear injury.
- LDL: Abnormally low. Note that individuals with severe hyperacusis may be unable to tolerate an LDL test.
Misophonia
- Emotional/behavioral reaction to specific trigger sounds.
- Common triggers: chewing, sniffing, pen clicking, throat sounds.
- Responses include anger, disgust, or panic.
- Loudness is not a factor ─ context is.
- LDL: Typically normal.
Phonophobia
- Anxiety or fear in anticipation of sounds.
- May arise from prior painful experiences or anxiety disorders.
- Often co-occurs with migraines.
- Leads to avoidance of sound environments.
- LDL: Often normal, distress is psychological rather than auditory.